If you have been told you may have breast hypoplasia, or insufficient glandular tissue (IGT), you may be feeling uncertain about what this could mean for breastfeeding.
Many parents have never heard of hypoplasia. It is also something that many healthcare professionals may rarely come across in clinical practice simply because it is relatively uncommon.
I have written this guide to help explain what breast hypoplasia is, how it may affect breastfeeding, and why early feeding support can be particularly important. Some parents also find it helpful to share this information with their midwife during pregnancy or after birth to help guide conversations and feeding plans.
Importantly, having features associated with hypoplasia does not automatically mean you will be unable to breastfeed or make milk. Every breastfeeding journey is individual, and many parents with hypoplasia go on to have meaningful and positive breastfeeding relationships with their babies.
What Is Breast Hypoplasia?
Breast hypoplasia, sometimes called insufficient glandular tissue (IGT), refers to breasts that may not have developed the typical amount of milk-producing glandular tissue.
Milk-producing tissue develops during puberty and pregnancy. In some people, the breasts may contain less glandular tissue than expected, which can affect milk production after birth.
Hypoplasia is not related to breast size. Small breasts can make a full milk supply, and larger breasts can still have reduced glandular tissue. Breast appearance on its own cannot confirm how much milk someone will or will not make.
For some parents, hypoplasia may have little or no impact on feeding. For others, it may contribute to a lower milk supply despite frequent breastfeeding, good attachment, and ongoing feeding support.
How Common Is Breast hypoplasia
Breast hypoplasia is considered relatively uncommon.
Even among professionals who regularly support breastfeeding families, it may not be encountered often. As a midwife and breastfeeding specialist, I have worked with only a small number of families affected by hypoplasia over many years in practice.
Many midwives provide excellent general breastfeeding support but may not have had specific education around hypoplasia or insufficient glandular tissue so they may be unfamiliar with it.
Lactation education beyond basic breastfeeding training is often undertaken separately through additional study and clinical experience. This is one reason why some parents find it helpful to bring information about hypoplasia to appointments so that feeding support can be planned collaboratively and individual needs recognised early.
Signs That May Suggest Hypoplasia
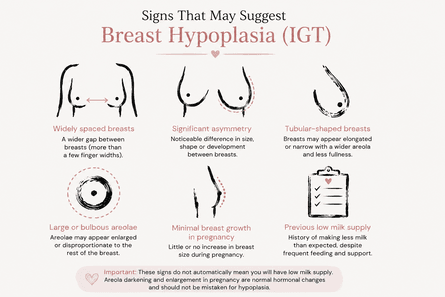
There are some breast features that may be associated with hypoplasia. These can include:
- breasts that are widely spaced
- significant breast asymmetry
- tubular-shaped breasts
- enlarged or bulbous appearing areolae
- very little breast growth or breast change during pregnancy
- previous experiences of unexpectedly low milk supply
Some parents describe their breasts as having a “tubular” shape or noticing that the areolae appear disproportionately large or prominent compared with the rest of the breast tissue. These signs do not automatically mean someone will have difficulties breastfeeding or making milk.
It is also important to remember that areola darkening and enlargement during pregnancy are very normal hormonal changes and, on their own, should not be mistaken for hypoplasia.
Some parents with several of these features go on to make a full milk supply. It is often only after birth, once feeding begins and milk production increases, that a clearer picture develops.
What Might This Mean for Breastfeeding?
Breast hypoplasia can affect breastfeeding in different ways.
Some parents will make a full milk supply. Others may make most, but not all, of the milk their baby needs. Some may require supplementation from early on despite frequent feeding and appropriate support.
This can feel emotionally difficult, particularly for parents who had hoped to exclusively breastfeed. It is important to understand that reduced milk production associated with hypoplasia is not caused by a lack of effort, motivation, or wanting breastfeeding “enough”.
If supplementation becomes necessary, this does not mean breastfeeding has failed. Your baby can still benefit from receiving your milk, regardless of quantity, and many families continue to have positive and rewarding breastfeeding relationships alongside supplementation.
Breastfeeding is about far more than nutrition alone. Time at your breast can continue to provide comfort, closeness, regulation, skin-to-skin contact, and emotional connection for both you and your baby. Many parents find breastfeeding remains an important part of bonding and settling their baby even when additional milk feeds are needed.
For some families, breastfeeding may continue for comfort, connection, overnight settling, or emotional reassurance long after supplementation has become established.
For many parents with hypoplasia, the goal becomes protecting and supporting the breastfeeding relationship alongside ensuring your baby is feeding well and growing appropriately.
Breastfeeding can feel overwhelming — but you don’t have to work it out alone.
If you’d like calm, practical guidance with feeding, positioning or common challenges, I offer video consultations and face-to-face breastfeeding support in and around Putney, South West London.
You can also explore my Online Breastfeeding Course for clear explanations of how feeding works and how to manage common problems.
Why Early Feeding Support Matters for Breast Hypoplasia
When breast hypoplasia is suspected, early feeding support can be especially important.
This may include:
- close assessment of feeding and milk transfer
- responsive and frequent breastfeeding
- monitoring nappies, weight, and feeding behaviour
- expressing milk where appropriate
- making individualised feeding plans if supplementation is needed
- using paced feeding methods when bottles are introduced
Milk production can vary significantly from person to person, so feeding support should always be individualised rather than based on assumptions about what feeding “should” look like.
Early support can also help families feel more prepared, supported, and confident during the early days after birth, particularly if supplementation becomes part of their feeding journey.
Planning Breastfeeding Support With Breast Hypoplasia
If you already know you have hypoplasia from a previous feeding experience, or if you are concerned you may have it, it can be very helpful to discuss this during pregnancy rather than waiting until feeding difficulties arise after birth.
Many NHS trusts have infant feeding teams, and these professionals are often very familiar with supporting families affected by hypoplasia and low milk supply. Even simply being known to the team before birth can make it easier to access support quickly once your baby arrives.

Some parents also choose to seek support from an independent breastfeeding specialist or infant feeding professional antenatally.
These conversations can provide space to discuss:
- previous feeding experiences
- feeding goals and expectations
- feelings around supplementation
- protecting the breastfeeding relationship
- expressing and colostrum harvesting
- paced feeding approaches
- appropriate supplementation volumes if needed
- plans for feeding support after birth
Having these discussions before birth can help parents feel more informed, emotionally prepared, and better supported as they begin their feeding journey.
Emotional Feelings around Breast Hypoplasia
Concerns about milk supply can bring a great deal of anxiety during pregnancy and early parenthood.
Parents with hypoplasia often describe feelings of guilt, fear, disappointment, or pressure, particularly if breastfeeding does not unfold as they had hoped.
Compassionate, realistic support matters.
Feeding your baby is not measured only by ounces of milk. A breastfeeding relationship can still be deeply valuable and meaningful even if supplementation is part of your journey.
Final Thoughts
Breast hypoplasia is relatively uncommon, and many parents will never hear the term.
If you think you may have hypoplasia, early support, realistic preparation, and individualised feeding guidance can make a significant difference. Understanding your options before birth can help you feel more informed and supported, whatever your feeding journey looks like.
Most importantly, breastfeeding does not need to be all or nothing to be worthwhile. Feeding journeys can look different from family to family, and support should always centre on both the wellbeing of your baby and your wellbeing as a parent.
If you would like individual breastfeeding support during pregnancy or after birth, you are welcome to contact me so we can discuss your circumstances. Some parents find that having a personalised feeding plan and specialist support before birth helps them feel more confident and emotionally prepared for the early weeks with their baby.




